Misconceptions about ivermectin dosing
It's quite a wormhole

Quick intro to ivermectin
Ivermectin is a broad spectrum drug that’s been widely used as an antiparasitic for decades. Since 2012, there have been multiple studies indicating that it has antiviral properties as well. For a few examples, see here, here, here, or here. More recently, it has been studied as a treatment for COVID-19 (see here).
Its use in treating COVID-19 has been controversial, to say the least. In fact, if you only read mainstream articles about it you might come away with the impression that it’s a livestock or “horse dewormer,” despite the fact that it’s a Nobel prize-winning drug on the World Health Organization’s list of essential medicines and has been administered billions of times to humans.
I’ll get back to people’s perceptions of ivermectin later, especially in the media.
The main focus of this article will be to examine an argument against it that I’ve come across again and again: that ivermectin could not possibly work against COVID because the dosage required to have antiviral activity is not achievable in humans.

An in vitro study that started a mini meme
An “in vitro” study involves testing cells in culture, like in a test tube or petri dish. It’s a useful type of study because it allows one to study cells in a highly controlled environment.
However, their results need to be taken with a grain of salt, because conditions in a test tube are not at all the same as physiological conditions within an organism.
In June 2020, an in vitro study by Caly et al., used Vero-hSLAM (African green monkey kidney) cells to test antiviral activity of ivermectin against SARS-CoV-2. In this study, they took infected cells and added ivermectin at different concentrations and measured if there was any reduction in viral RNA.
The IC50, which is the concentration of a drug resulting in 50% inhibition, was determined to be ~2 μM under these conditions. They also reported that 5 μM ivermectin resulted in a 99.8% reduction in cell-associated viral RNA after 24 h.
Thereafter, “2 μM” or sometimes “5 μM” or the equivalent “ 5 µmol/L” concentration, was mentioned in several papers and criticisms as the concentration of ivermectin in plasma that would be necessary to inhibit SARS-CoV-2.
The meme spreads doubts on dosage
For example, in this paper by Momekov et al., a literature survey of published dose regimens of ivermectin was performed to try to determine the maximum concentration found in plasma among humans, what they call “Cmax” below:
The analyzed data show that, at least at the clinically relevant dose ranges of ivermectin, the published in vitro inhibitory concentrations and especially the 5 µmol/L level causing almost total disappearance of viral RNA are virtually not achievable with the heretofore known dosing regimens in humans.
The 5 µmol/L concentration is over 50 times higher than the levels attainable after 700 μg/kg and 17 times higher vs. the largest Cmax found in the literature survey (247.8 ng/ml)
And in this study by Schmith et al., they used a pharmacokinetic model to try to predict what Cmax would be in the plasma, and used data on the plasma:lung ratio found in cattle to try to determine the achievable level in lungs. They also concluded that ivermectin was unlikely to reach the IC50 as reported by Caly et al., which was assumed to be the dosage required.
Responses to the doubts on dosage
In this video, the PI (principal investigator) for the Caly et al. study, Kylie Wagstaff, responds to the criticisms and explains why it’s a fallacy to use their assay to determine the effective dose in humans:

Lung concentrations
In her presentation, Wagstaff points out that lung cells would theoretically accumulate higher concentrations of ivermectin compared to plasma.
In a screenshot of her presentation below, the red line on the far right is what a modeling study by Arshad et al., predicts for the achievable concentration in lungs, while the red line on the far left is the range predicted by Schmith et al., which was mentioned earlier. The dotted blue line is supposed to be the average of the models (note: the horizontal axis is on a log scale).

The reason we are relying on modeling studies is that there are no direct measurements of the maximum achievable lung concentrations of ivermectin in humans.
I can’t speak to why the two modeling studies have such different predictions, or which is better, but any honest conversation about dosage should acknowledge that there are different theoretical predictions.
[UPDATE 3/4/22: Here’s another modeling study. This one predicted lower lung concentration than in the Arshad et al. study. And here’s a study that looked at biodistribution of ivermectin in different tissues. This one showed lung concentrations were roughly 22-fold higher than what was found in blood.]
No innate immune response
Wagstaff also points out that the IC50 of 2 μM that they found was particular to the cells they used in their assay, Vero (monkey kidney) cells.
She makes the point that the Vero cells used in their assay do not release interferons, which signal to surrounding cells that a viral attack is occurring. So if their assay had been done in cells that did release interferons, we could imagine that the effect of ivermectin would be greater, or we’d see the same effect but at a lower concentration.
Another way to put it would be that if ivermectin helps prevent the virus from suppressing the host cell’s innate immune response, then it would allow infected cells to release interferons, which could lower the total virus being produced from the entire cell culture.
No lymphocytes, myeloid, or adipose cells
Wagstaff doesn’t mention this in her presentation, but the tissues used in their assays also do not include myeloid cells or lymphocytes, which are important for mounting immune responses against viral infections, or adipose (fat) tissues in the lungs, which can release inflammatory signals (more on this later).
The posited mechanism of action
Wagstaff posits that one of the mechanism of action of ivermectin is as a host-acting agent, so its specific effect (and effective concentration) would vary by the type of cell being studied.
In order to make copies of itself, the SARS-CoV-2 virus needs to import some of its proteins into a host (infected) cell’s nucleus. This would allow the virus to hijack the cell’s machinery and suppress the host’s innate immune response, such as the release of interferons.
Proteins, however, can’t just enter the nucleus willy nilly; they need to be “shuttled” into the nucleus with the help of host cell proteins called importins, which consist of importin-α and importin-β subunits.
Wagstaff posits that ivermectin binds to importin-α, which would prevent viral (as well as host) proteins from entering the nucleus (more here).

Something that Wagstaff does not discuss in her presentation, but is relevant to this discussion, is that if the mechanism of action is as she describes, it stands to reason that the efficacy of the drug in a specific tissue might depend on the expression levels and types of importins in that tissue.
Not only do different tissue types have different types of importin-α (of which there seem to be several), but the levels of importin-α proteins vary depending on the tissue. This study looked at several different forms of importin-α protein in different human tissues:

Importin α3, importin α4, hSRP1, and RCH1 are each different types of importin-α proteins (they’re the products of different genes), and each band you see in the image is supposed to be importin-α protein. The darker the band is, the more protein was in the tissue.
Moreover, sometimes there was more than one band for a given importin-α type. Maybe these correspond to different post-translationally modified versions of the protein, or to products of alternatively spliced mRNAs.
So if at least part of ivermectin’s mechanism of action has to do with its binding to importin-α, the drug’s effect could vary widely depending on the amount of importin-α, as well as the specific type or post-translational modifications of importin-α in that tissue.
By the way, this study by Segatori et al., showed that concentrations as low as 0.2 μM reduced importin-α transport into the nucleus by about 20% in both Vero and Hela (human cervix adenocarcinoma) cell lines.
Other possible mechanisms of action
It should be mentioned that there are several other putative mechanisms of action for ivermectin that are in discussion, which you can read about here.
Ivermectin has a macrolide structure (more on macrolides later), and macrolide compounds in general, are known to exhibit extremely diverse actions.
But ivermectin binds to plasma proteins
I’ve also heard some people make the claim that because ivermectin binds to plasma proteins like albumin, this makes some of the ivermectin unavailable; aka takes it “out of circulation.” In other words, the implication is that only unbound drug in the plasma could have a therapeutic effect.
However, any drug that is in the plasma, or the liquid portion of the blood, would presumably be in equilibrium with what’s bound to proteins. This means that if any ivermectin in the plasma gets taken up by cells, this would lower the concentration in the plasma, which might mean some of what’s bound to proteins would then get released into plasma.
In fact, one of the studies that found that ivermectin binds to plasma proteins, said:
It is clear that ivermectin has an extended pharmacodynamic potential because of its avid binding to plasma proteins; other drugs or diseases states may modify this slow release and extended action of ivermectin.
So they speculate that ivermectin’s binding to plasma proteins could result in some kind of slow release effect.
At the very least I think we can say that we currently don’t know the fate of any ivermectin that is bound to plasma protein.
In vitro studies in human lung tissues
Can in vitro studies in lung tissues tell us anything? As far as I can tell, there were three in vitro studies that looked at the effect of ivermectin in human lung cell lines that were infected by SARS-CoV-2.
The first, by Jitobaom et al., found that the IC50 for ivermectin in Calu-3 cells, which are derived from a human lung cancer epithelial cell line, was 0.2 μM. This study also reported that the IC50 in Vero E6 (monkey kidney) cells was 1.23 μM, which was similar to what the Caly et al. study found.
The second, by Chable-Bessia et al., also looked at Calu-3 cells, as well as human pulmonary alveolar A549-hACE2 cells, which were engineered to express the human receptor ACE2. The IC50 in Calu-3 cells that they reported, 3.36 μM, was higher than what was reported in the first study. The IC50 was 2 μM for the A549-hACE2 cells.
The third study, by Kumar et al., found an IC50 of 5.8 μM for Vero E6 (monkey kidney) cells. Then they looked at both Calu-3 and PBEC cells, which are primary bronchial epithelial cells, but instead of trying to determine the IC50 they tried 5 μM and 10 μM in the case of the Calu-3 cells, and 10 μM of ivermectin in the PBEC cells. In both the Calu-3 and PBEC cells, they didn’t find that ivermectin had a significant antiviral activity at the concentrations given.
As mentioned earlier, we don’t know what concentration is achievable in human lungs, so we can’t say whether the concentrations used in these studies are realistically achievable in living breathing lungs, though they were within the range predicted by the Arshad et al study.
Something that all the studies had in common was that they all looked at Calu-3 cells, but the first reported an IC50 of 0.2 μM, the second reported 3.36 μM, and the third did not find antiviral activity with 5 μM or 10 μM.
I can’t speak to why these studies had such varying results. But these studies show how results can vary even among experiments with the same cell line. It’s possible that this cell line has diverged over time. Obviously there were also variations in the protocols used.
The lung cells used in these assays were probably better models for what actually goes on in the lungs compared to Vero (monkey kidney) cells; they can at least exhibit some innate immune responses. However, even Calu-3 epithelial cells, which apparently were first isolated in 1975 from a 25-year-old Caucasian male, exhibit different immune responses compared to freshly isolated epithelial cells.
And just as with the assays done in the Vero cells, these lung tissue assays didn’t include myeloid cells or lymphocytes, which are important for mounting immune responses against infections, or adipose (fat) tissues, which will be discussed next.
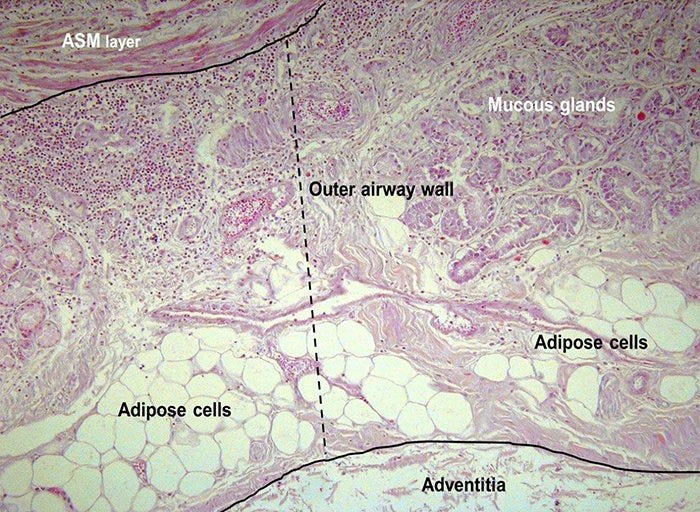
Why aren’t we talking about ivermectin in fat tissue?
The highest concentrations of ivermectin is reached in adipose (fat) tissues.
Given this, it’s surprising that no one has proposed that part of the efficacy of ivermectin, if any, could be directly within fat tissue, especially since:
We have evidence that SARS-CoV-2 infects fat tissue.
Fat tissue is present in the lungs, and fatter people have more fat tissue in their lungs.
SARS-CoV-2 infected patients who are overweight have poorer outcomes (see here, here, here and here).
Incidentally, for a given BMI, males have more fat tissue in their lungs and also suffer from poorer outcomes from COVID-19, compared to females.
Fat tissue can produce proinflammatory cell signaling molecules such as leptin, interleukin-6 (IL-6), and tumor necrosis factor alpha (TNF-α). According to this study, SARS-CoV-2 infection of visceral fat led to an increase in leptin production, which would add to the pre-existing chronic inflammation that tends to occur in obese people.
So someone should explore the degree to which ivermectin could be acting directly on fat tissue, including in the lungs.
There are historical precedents for this kind of confusion
Macrolides are antibiotics that contain a large macrocyclic lactone ring to which one or more deoxysugars may be attached. As mentioned earlier, ivermectin, which is a macrocyclic lactone, has structural similarities to these drugs.
It took awhile to understand the pharmacokinetics of macrolides, like azithromycin, which is used to treat certain bacterial infections. In fact, they were originally dismissed because blood levels appeared too low to have efficacy, but clinical results showed that they had an effect in bacterial infections.
As it turns out, their concentration in epithelial lining fluid generally greatly exceeds what’s in the plasma, and there is evidence that they can concentrate in white blood cells, and drug-laden white blood cells can even deliver loads of drug directly to infection sites (see here and here).
Just to be clear: drug that is within blood cells, or any cells, would not be measured in plasma, since plasma is essentially all the components of blood minus the cells.
Even when it comes to ivermectin, no one seems to dispute its efficacy as an antiparasitic against worms like microfilariae, and yet its pharmacokinetics as an antiparasitic does not seem to be 100% clear.
From a review on ivermectin from 2017:
Ivermectin’s mode of action against parasites in the human body remains to be clarified. There is a substantial disparity between maximum plasma concentrations after ivermectin administration and the concentrations needed to induce paralysis in microfilariae.
That review also mentions that parasites are not necessarily killed when plasma drug levels are at their highest. Moreover, antiparasitic activity could be found for at least a month after a single dose of ivermectin, even when pharmacokinetic calculations suggest that ivermectin should no longer be detected by conventional methods (see here and here). This has led some to speculate that its activity could be due to drug-induced changes in the host immune system.
Going back to COVID-19, people have argued that dosing in humans could not possibly lead to the antiviral effects seen in vitro. But when we consider the type of cells affected, and the synergy between ivermectin and the immune system, claims of impossibility were certainly premature.
Obviously there’s still a lot to be discovered about ivermectin’s mode of action.
So ultimately even if we don’t completely understand the pharmacokinetics or modes of action of a drug, if clinical or real world data suggests that a drug has an effect, we should not ignore that.
The state of the RCTs
So what does clinical or real world data say?
I won’t go over all the evidence for ivermectin, because there’s a lot, but I’ll go over some of it, starting with what’s gone on surrounding the discussion around the RCTs (randomized controlled trials).
The ivmmeta site reports that those given ivermectin for COVID-19 saw statistically significant improvements compared to controls, and to date it links to 80 studies, including observational studies, randomized controlled trials (RCTs), and systematic reviews.
In Nov 2021, Scott Alexander wrote a piece on ivermectin that many thought was the “final word” on the ivermectin RCTs. In a nutshell, Scott Alexander went through all the RCTs to date and determined that some should be excluded because of either fraud or methodological issues, and after excluding those, he found an effect in favor of ivermectin, though it wasn’t statically significant. When he changed the endpoints he used for each study, he ended up with a borderline statistically significant effect.
In the end, he thought that there did seem to be a signal among the noise, but that in so far as there was a signal, it could just be due to ivermectin’s action against worms. In other words, the studies that showed the most positive effect for ivermectin were done in countries that he thought would have a high prevalence of parasitic worms in the population, so he thought the ivermectin was killing people’s worms, which would allow them to better fight off COVID.
In response to his piece, Alexandros Marinos wrote an analysis that did multiple meta-analyses using different combinations of studies, including ones that used Scott’s exclusions. He found that with all the combinations, we still found a positive effect, within the bounds of “statistical significance,” though with varying confidence intervals, and Scott’s own analysis didn’t actually move the conclusion much from what ivmmeta.com showed, even though Scott had excluded almost half the studies.
To my knowledge Scott has not adequately responded to this analysis; see Scott’s response here.
Regarding the “worms hypothesis”- I’m not saying that ivermectin’s effect on worms can’t have anything to do with the signal we see in the COVID-19 studies, but this is just a hypothesis that needs to be tested at this point. Nobody actually measured the prevalence of worms in the participants of the ivermectin studies.
And yet smug talking heads like Robby Soave of Reason Magazine, and journalist Ryan Grim talked about it like it’s something that “we all know” to be true:
Here’s what Ryan Grim said:
We understand now what happened with ivermectin. Ivermectin, you know, basically deals with worms. And so, when they were giving it to people in Bangladesh, in Asia…
Then Robby Soave jumped in:
It was helping cause it was killing off the worms they had, which made their body better able to fight COVID.
As Alex Marinos put it, “Narrative beats data every time with these professional pundits.”
Speaking of narrative, more recently there was a paper in JAMA that showed that those who got ivermectin had a lower death rate than controls, but for some reason they obfuscated that in their paper.
And we’re still waiting on the results of the large TOGETHER trial, although that hasn’t prevented people drawing conclusions about it based on some slide decks:
Later I’ll discuss why the conversation surrounding ivermectin has gotten so confusing, or as I would argue, derailed.
We’re definitely dosing suboptimally
So there does appear to be signal among the noise, though people disagree over how significant it is, or whether it’s just because of some effect on worms.
It needs to be said that on top of that signal, any studies on ivermectin likely understate its efficacy, because most studies are probably giving the drug suboptimally.
This is because there are many more ways to get drug administration wrong, than right.
To illustrate that, I’m going to steal an image from the Rounding the Earth Substack. This image was for hydroxychloroquine, but we could easily apply it to ivermectin:

The true optimal protocol lies in a rather small area in this space; therein lies an optimal dose, timing (when the drug is given- either before or after infection or symptom onset), and set of conjunctive therapies (other medicines or vitamins or minerals that would work with it synergistically).
Here are just a few factors that might matter when it comes to dosing or absorption:
Obviously too little drug could be given.
It could also be given too late in the course of infection.
Sex, age, and physiological status can all influence pharmacokinetics.
In a small study done with 16 humans, it was even found that orange juice decreased the bioavailability of ivermectin.
The mode it’s given in matters, whether it’s tablets, ethanol solutions, etc. People with malabsorption issues might not be absorbing much from oral forms. Here’s an example of someone who had to get ivermectin given via an injection for their case of strongyloidiasis, because they had severe malabsorption issues.
Small repeated doses might be more effective than a single large dose.
Many studies can’t even get the timing right and give ivermectin too late during the course of an infection. So it’s hard to imagine that we are seeing the full extent of its efficacy, if it is effective.
What gets lost in the RCTs
Some people will only consider the RCTs when looking at all the evidence for ivermectin.
RCTs are great when designed and done well, but they have their weaknesses, and unfortunately are gameable. For more on that see here, here, and especially here.
I will say that I personally put a fair amount of weight in testimonials from doctors who have treated lots of COVID patients with ivermectin. After treating hundreds or even thousands of patients, they would develop a sixth sense for what works, and are also the experts at administering the drug.
Moreover, I’ve heard from clinicians who have described the dynamics of how sick patients that were on a downward trajectory quickly reversed course after treatment with the drug. That kind of information easily gets lost in a paper describing an RCT. It’s also not easily quantifiable.
Under narrow definitions of evidence, that kind of information gets dismissed as “anecdotal.” As if anecdotes, especially repeated over and over again from multiple different sources, are not evidence.
It’s also astounding to me that some people are so sure that ivermectin doesn’t work, despite the fact that the doctors who were using it seem to have the best track records, aka the least number of COVID-19 patients lost, and multiple doctors around the world seemed to independently come up with ivermectin as a therapeutic against COVID-19.
Now of course it’s possible that they were all influencing each other. We’ve seen situations before where groups of highly intelligent people can end up in groupthink.
I can’t say for certain that this isn’t happening here, but at the very least, can we agree that it makes no sense that doctors should be banned from prescribing ivermectin, especially given how safe it is?
UPDATE 3/5/22: Here’s more on ivermectin’s safety:
Also think about all the scrutiny that ivermectin has been under; even after all that, we still see a signal in the data. Are we even applying half that amount of scrutiny to the COVID vaccines?
Even if we all agreed that we aren’t sure ivermectin worked, are we going to refrain from giving it to sick people, because it “might not work”?
Here’s one way to put it:

It especially doesn’t make sense that some doctors were threatened with losing their jobs or licenses for prescribing ivermectin for COVID.
Again, how does this make any sense, given the length of its safety track record, which by the way is several decades longer than what we have for the vaccines?
An observation about the ivermectin conversation
Although I can’t know for sure whether ivermectin has an effect on COVID-19, I will fully admit that I am biased in that I make an extra effort to analyze its criticisms.
Why? Because there is evidence that there are dishonest actors that have tried to derail the ivermectin conversation.
First there was the unbelievable amounts of propaganda painting ivermectin as “horse dewormer,” including from our very own FDA:


More on the propaganda here and here.
Then I saw how researcher Andrew Hill, who had ties to an organization with conflicts of interests, was caught on camera admitting that he was being pressured to downplay the evidence for ivermectin in one of his papers, even though he thought the data showed that it worked. He also admitted that someone from his sponsoring organization, who was not an acknowledged co-author, wrote the conclusion for his paper. For more on that see here.
[UPDATE 3/4/22: Dr. Tess Lawrie and others, have since made an incredible video plea to Andrew Hill. In that video, Hill also talks about the organization that was pressuring him to change his conclusion (Unitaid). Watch here.]
Why is this happening? Well it’s speculated that because ivermectin is a cheap generic drug, it would get in the way of powerful, corporate interests, like expensive patented treatments that would make pharma lots of money.
Regardless of the reasons, these shenanigans have derailed the ivermectin conversation.
Just look at the level of misconception displayed by someone who’s considered a public health expert, Paul Offit. Offit is internationally recognized as an expert in vaccinology and virology, and regularly serves on vaccine advisory committees for the FDA. Here he discusses ivermectin for the treatment of COVID:
About ivermectin, he said: “talk to your large animal veterinarian” and “to date there’s no data” and “it’s interesting how people who won’t get a vaccine are perfectly willing to take hydroxychloroquine or ivermectin, which can be harmful” and “certainly there’s not evidence that it’s helpful.”
Again, ivermectin is an incredibly safe drug, and in some countries it’s available over the counter.
Offit was completely dismissive. I’m not saying he’s a bad guy, but he has not been getting good information on this.
In fact, because of the propaganda surrounding ivermectin, supporting ivermectin hurts your respectability.
This means that a lot of the people with the the most domain-level knowledge on the issues discussed in this article, like pharmacology, are probably not even bothering to look at the weaknesses in the arguments against ivermectin, because they’ve heard that it’s a “horse dewormer.”
That obviously hurts our prospects for finding out the truth about it.
Early treatments in general
Lastly, I should mention that that when it comes to Omicron, I’ve heard anecdotally that hydroxychloroquine works better than ivermectin.
Sadly, we saw sketchy things happening surrounding the conversation around hydroxychloroquine as well.
Like ivermectin, it was attacked in the media, especially after Trump talked about it. We even saw fraudulent or rigged papers get published to make hydroxychloroquine look bad. See here or here to read about a fraudulent paper that was published in The Lancet, or here for an example of a trial that was designed to fail.
If you want to learn more about the saga of hydroxychloroquine, see the deep dives that statistician Mathew Crawford did here, here, and here.
And for more on what happened to early treatments for COVID-19 in general, see here:
Even if it’s true that ivermectin was more effective on previous strains, before the emergence of Omicron, it’s still important to get to the truth about it.
After all, if it turns out that Big Pharma interests and propaganda were able to prevent life saving treatments from getting to the public, who’s to say this won’t happen again in the future?
And where else is this kind of malfeasance occurring now?
If you’d like to see more of this kind of article, you can subscribe or follow here for updates.
Another outstanding piece. Thank you!! Glad to be a paying subscriber of your work.
If someone else hasn't asked this, would you mind providing in the piece some references for Andrew Hill's conflicts of interest related?