

A timeline of how vaccine efficacy devolved
And how our nonsensical health policies continued anyway

In March 2021, CDC Director Rochelle Walensky said “vaccinated people do not carry the virus,” and in May 2021, Anthony Fauci said that vaccinated people “become a dead end to the virus.”
But as 2021 went on, it became increasingly clear that the COVID-19 vaccines were not very efficacious at preventing infection, and vaccinated people could still transmit the virus. Despite this, governments around the world enacted draconian measures to coerce people into getting vaccinated.
This article will present a timeline of how vaccine efficacy against infection or high viral load (virus levels in the nose) waned over time, and how our health policies reacted, or failed to react, to changing information.
Consider this a record of how things went down during a particularly confusing time.
It’s possible for injected vaccines to affect virus levels in the nose or lungs
Before the emergence of SARS-CoV-2, there was evidence that injected vaccines could produce a mucosal response to a respiratory virus. They won’t produce the same kind of mucosal response an infection would, but they could produce a response that lowers viral load in the lungs, and to a lesser extent, the nose.
For more on that, see this: Parenteral Vaccination Can Be an Effective Means of Inducing Protective Mucosal Responses
“Parenteral vaccination” means the vaccine was given by routes other than the digestive tract, and would include intramuscular, intravenous, and subcutaneous injection.
Also, before the emergence of SARS-CoV-2, we had studies of injected vaccines against SARS-CoV showing that they could lower virus levels in the lungs. Here’s one example: A DNA vaccine induces SARS coronavirus neutralization and protective immunity in mice

Early on, the COVID-19 vaccines did seem to lower viral load somewhat
Turning to vaccines against SARS-CoV-2, there was evidence that they could help lower viral loads, especially in 2020 and early 2021.
Before we get into that, it should be mentioned that many of the studies use Ct values1 of PCR tests as proxies for viral load. It’s arguable that this is problematic. However, for the purposes of this article, we’ll play along.
Animal studies
The earliest evidence that the vaccines could reduce SARS-CoV-2 viral load was in animal studies.
For example there was this paper on the AstraZeneca vaccine: ChAdOx1 nCoV-19 vaccine prevents SARS-CoV-2 pneumonia in rhesus macaques
In that study they exposed rhesus macaques (monkeys) to SARS-CoV-2 virus and found that intramuscularly vaccinated monkeys (red or blue) had lower viral RNA in their BAL (bronchoalveolar lavage) fluid, which contains fluid from the lower respiratory tract, compared to unvaccinated monkeys (green):

However, viral RNA in the nose was not that different between vaccinated and unvaccinated monkeys:

Then there was this paper about the Moderna vaccine: Evaluation of the mRNA-1273 Vaccine against SARS-CoV-2 in Nonhuman Primates
This study also exposed rhesus macaques to SARS-CoV-2 virus and compared viral levels between vaccinated and and unvaccinated. They also found lower viral RNA in BAL fluid of the vaccinated, compared to the unvaccinated group (A below):

Compared to unvaccinated, they also found lower virus levels in the nose in the group that got higher dose of the vaccine (B above). However, note that there were still a few vaccinated individuals that had levels of virus that were comparable to unvaccinated individuals.
Other animal studies showed injected vaccines having some effect on viral loads, especially in the lower respiratory tract (see here, here and here).
The Vaccine Trials
In December 2020, the NEJM published interim results from the Moderna and Pfizer trials (see here and here). These showed impressive-looking efficacy against “prevention of COVID-19 illness,” and were used as the basis for applying for emergency use authorization.
Now, I would understand extreme skepticism towards some of these results, especially Pfizer’s. Among other things, when calculating efficacy they ignored cases of “suspected covid-19” where people had symptoms, but were not PCR confirmed (more on that here). This category of people was 20 times larger than PCR “confirmed” cases, and including these people would have drastically decreased the calculated efficacy. Then there was the fact that individuals were excluded for unknown reasons, especially from the vaccine group. Oh, and a whistleblower reported fraudulent behavior in at least one of the trial sites.
However, for the purposes of this article, we’ll take their results at face value and say that they seemed to show high efficacy at “prevention of COVID-19 illness.”

Other Studies
Then there was this observational study out of Israel, which compared vaccinated vs. unvaccinated people who had tested positive using PCR: Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine
They sampled people between December 2020 - February 2021 and found that viral load was reduced for infections occurring 12–37 d after the first dose of vaccine.

Then there was this study: Single dose of a mRNA SARS-CoV-2 vaccine is associated with lower nasopharyngeal viral load among nursing home residents with asymptomatic COVID-19
They also sampled people between December 2020 - February 2021, and found that the vaccinated had reduced viral load compared to the unvaccinated:
A timeline of devolution
I’ll now present a timeline of data showing the decline of vaccine efficacy against infection or high viral load. Note: this is different from efficacy against severe disease or death, which didn’t devolve as quickly.
December 2020
December 2020 was when the COVID-19 vaccines first became available to certain segments of the population.
January 2021
Even as early as January 2021, there were hints that new virus variants could pose a problem for vaccine efficacy. To this, Anthony Fauci said:
What we likely will be seeing is a diminution… in what would be the efficacy in the vaccine-induced antibodies.
However, he said the vaccines could still be “effective,” and this gave us “all the more reason” to vaccinate people faster.
March 2021
CDC Director Rochelle Walensky said: “vaccinated people do not carry the virus, don’t get sick” (see here).
April 2021
Pfizer CEO Albert Bourla said people will “likely” need a booster dose of a Covid-19 vaccine within 12 months of getting fully vaccinated:
A likely scenario is that there will be likely a need for a third dose, somewhere between six and 12 months and then from there, there will be an annual revaccination, but all of that needs to be confirmed. And again, the variants will play a key role.
May 2021
In early May, there were reports of Seychelles experiencing a large rise in cases despite being the most vaccinated country in the world at the time, with 62% of its population fully vaccinated:

According to the Seychelles health ministry, more than a third of people who tested positive in the week of May 8 had been fully vaccinated. However they were using the Sinopharm or Covishield (AstraZeneca) vaccines. Maybe the vaccines used in the U.S. would hold up better?
On May 16, 2021 Anthony Fauci said (at around 3:30):
When you get vaccinated, you not only protect your own health and that of the family but also you contribute to the community health by preventing the spread of the virus throughout the community.
In other words, you become a dead end to the virus.
Around this time, statements from Rochelle Walensky indicated that she felt some “cautious optimism” given that “our case rates are coming down”:
we’ve done an extraordinary job in getting people vaccinated really quickly and now we have the hard work to do of getting more people vaccinated… And it is going to be in those people that we really need to get vaccinated and to keep our case rates coming down.
She also mentioned that the U.S. was planning for potential booster shots “just in case” (see here).
June 2021
In June 2021 a study from Greece came out where they had sampled 55 health care workers who had tested positive for SARS-CoV-2 between January - April 2021: Transmission of SARS-CoV-2 variant B.1.1.7 among vaccinated health care workers
They found that viral load, as measured by Ct values, did not differ between the vaccinated (all with the Pfizer vaccine), and unvaccinated. Furthermore, symptomatic infection was equally common in both vaccinated and non-vaccinated people.2

By late June, we also started to see a rise in cases in Israel, one of the most vaccinated countries (with Pfizer) at the time.
July 2021
By early July, we saw more hints from Israel that Pfizer vaccine efficacy against infection was devolving quickly:

This got a fair amount of media coverage at the time (see here or here).
Nevertheless, on July 21, 2021, Joe Biden said (see here at around 9:20):
You’re not gonna get COVID if you have these vaccinations
And on July 29, the Biden administration announced vaccine mandates for federal employees and contractors.
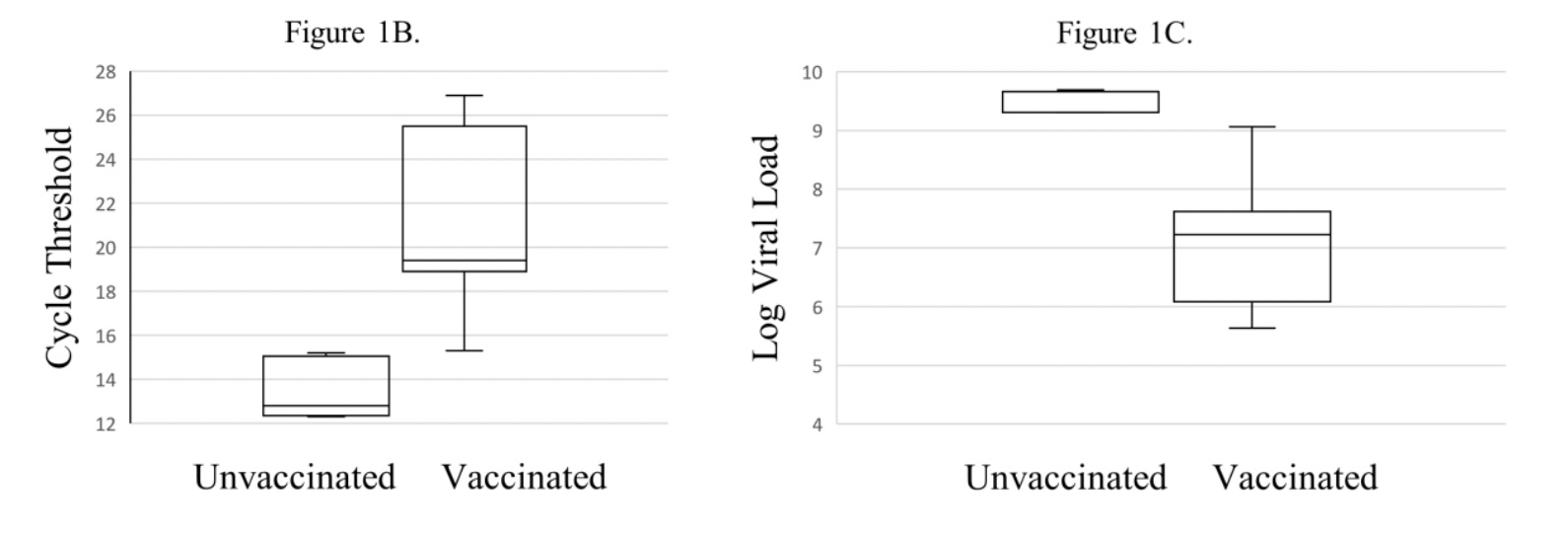
The next day, on July 30, 2021, the CDC reported a Covid-19 outbreak in Barnstable County, Massachusetts, where most of the residents were vaccinated. Viral levels, as measured by Ct values, were similar between vaccinated and unvaccinated people:

The very next day on July 31, 2021, this CDC-sponsored study was posted online as a preprint: Vaccinated and unvaccinated individuals have similar viral loads in communities with a high prevalence of the SARS-CoV-2 delta variant
That article went through a lot of versions. It was finally published more than a year later in September 2022, under a new title: Shedding of infectious SARS-CoV-2 despite vaccination.
Anyway, that study sampled 20,341 people who tested positive for SARS-CoV-2 from June- July 2021, and observed similar Ct values in the vaccinated and unvaccinated. Actually, the vaccinated had a slightly lower average Ct value. Remember, a lower Ct value indicates that there was more virus:

Note that the scale gets higher from top to bottom in the graph.
They also tested a subset of the samples to see whether the virus samples were infectious. 37 of 39 (95%) specimens from vaccinated individuals contained culturable, infectious virus, as compared with 15 of 17 (88%) specimens from unvaccinated people:

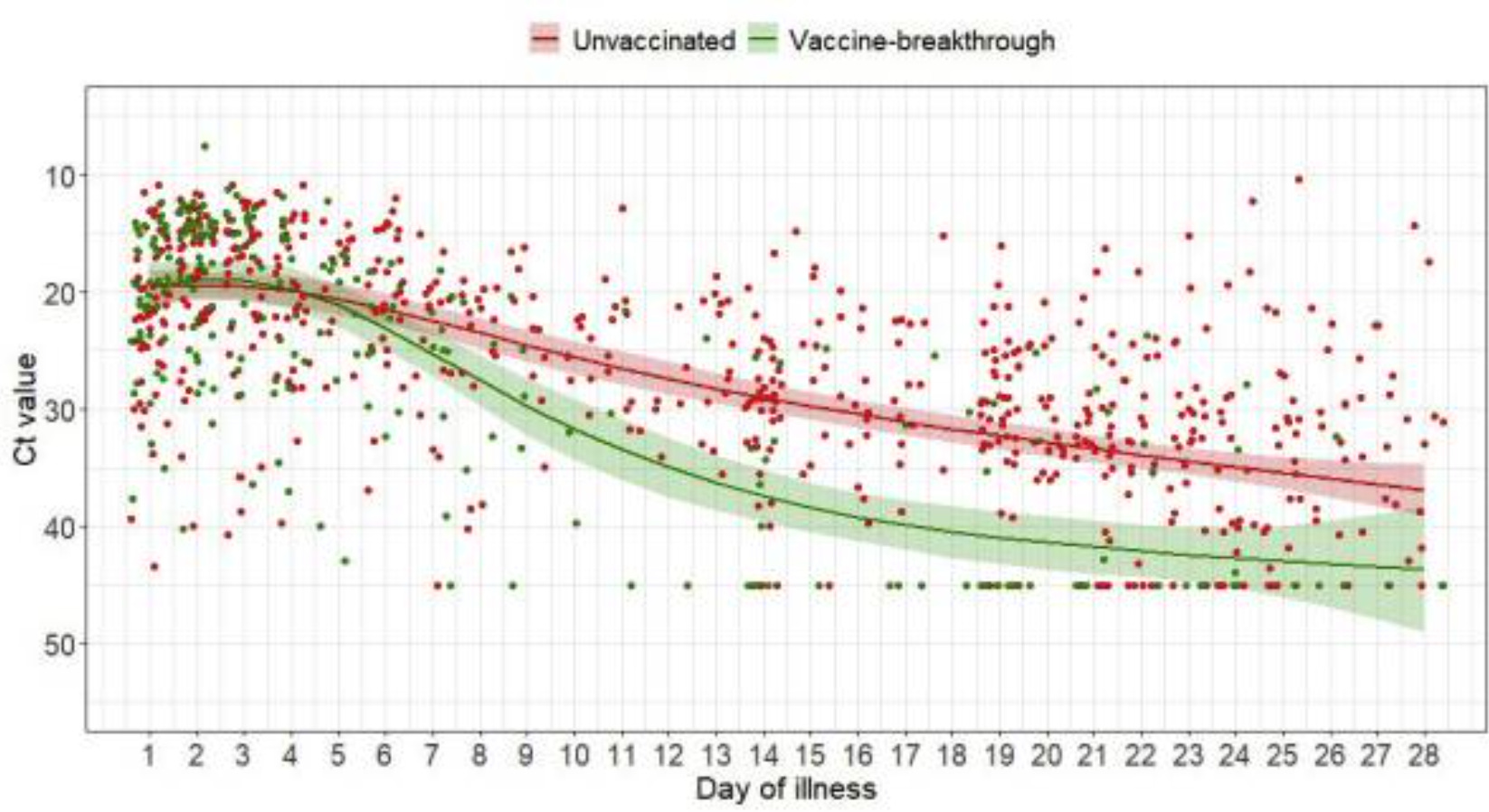
That same day (July 31, 2021), a study from Singapore came out as a preprint, though it would eventually be published in April 2022: Virological and serological kinetics of SARS-CoV-2 Delta variant vaccine breakthrough infections: a multicentre cohort study
That study sampled people who tested positive for SARS-CoV-2 between April - June 2021. They found that initial and peak viral loads3 were similar between the vaccinated and unvaccinated, though viral loads decreased faster in vaccinated individuals.
August 2021
On August 18, the CDC reported that vaccine efficacy against infection went from ~ 75% effective early on in the vaccination program (March-May 2021) to ~53% by June-July 2021 (see here).
That same day, the US announced it would begin a booster program in September.
On August 24, results from a massive study from the UK also showed that efficacy against infection was waning, and that infections in the vaccinated had similar peak viral loads as in the unvaccinated.
September 2021
This study came out in September 2021: Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States
It found that there appeared to be “no discernible relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days.” In fact, the trend line suggested a marginally positive association such that countries with higher percentage of population fully vaccinated had higher COVID-19 cases per 1 million people.

Now, this could have been explained by all kinds of confounders. But this didn’t look good.
Continuing Devolution
Throughout the rest of 2021 and into 2022, we continued to get more data showing waning efficacy against infection, as well as confirmation that vaccinated people had similar viral loads as the unvaccinated, and could transmit the virus (examples here, here, here, here, here, here).
November 2021
On November 4, 2021, the Biden administration announced vaccine requirements for businesses with 100 or more employees and health care workers.
A quick summary
Here’s a summary of some of the key statements or actions by health officials or politicians, along with some of the data just discussed (studies or findings are in blue):

Analyzing statements and actions by health officials
When Walensky said that “vaccinated people do not carry the virus,” or Fauci said that the vaccines make you a “dead end to the virus,” they were making sloppy and misleading statements.
Even the vaccine trials showed some vaccinated people getting infected, and animal trials before that had shown that even if vaccines could lower viral levels in the lungs, they were not as efficacious at lowering viral loads higher up in the respiratory tract, like the nose.
It would have been fine if they had said that vaccinated people carried less virus; we did have some studies showing that early on.
But even that had become debatable by spring of 2021, when the Greek study came out in June showing that vaccinated and unvaccinated who had been infected had similar viral loads.
However, that was a small study, so maybe no one was aware of it back then. But later in July, the CDC’s own data showed that vaccinated and unvaccinated people who got infected had similar viral loads. It also showed that vaccinated people could transmit the virus and cause outbreaks.
Despite this, the Biden administration, nonsensically, went ahead with vaccine requirements on federal employees and contractors. And even as more data rolled in confirming the CDC’s findings, the Biden administration escalated its vaccine policy in November of 2021 by expanding the vaccine mandates to healthcare workers and large businesses.
Trying to steelman the mandates
How could vaccine mandates possibly be justified, as late as fall 2021?
One could bring up the fact that vaccine efficacy against severe disease or death held up better than efficacy against infection or high viral loads. But arguably that was a private benefit, and the fact that vaccinated people could get infected and spread the virus meant that its public benefit was severely limited.4
One could make the argument that the vaccines still helped lower community virus levels; after all, the vaccinated seemed to clear virus faster if they did get infected, and there were studies suggesting that the vaccinated transmitted at lower rates compared to the unvaccinated (see here).
However, measuring transmission rates is challenging, and some of the data on transmission was mixed. But even if we granted that the vaccines helped reduce transmission, it was far-fetched at this point to think that we were going to control the spread of the virus anyway, as opposed to it becoming endemic.
Also: recall that the vaccine mandates didn’t make exceptions for those with natural immunity. That never made any sense; it never made sense to assume that those with natural immunity should be treated differently, as “virus spreaders,” any more than those who had been vaccinated.
One could have argued that even with waning efficacy against infection, the vaccines could still reduce the chances of getting infected, so it still made sense to make everyone get them. But efficacy against infection waned rapidly, in a matter of months:

That meant that unless people were willing to get boosted rather frequently, the most the vaccines could do was delay infection, which meant that every vaccinated person was destined to eventually become a virus shedder, unless they were willing to become hermits. This destroyed any rationale for segregating people based on vaccination status.
In a surprise twist, by the way, we now have some evidence of negative vaccine efficacy against infection (see here or here). Now, these results could just be due to sampling biases. But we shouldn’t rule out that unexpected things might be happening to people’s immune systems as a result of vaccination.
For example, according to this study, mice that were pre-exposed to LNPs5 were more resistant to flu but less resistant to the yeast Candida albicans. This is very surprising, and we should expect that we’ll continue to learn surprising things about the mammalian immune system.
The bigger point is that any certainty about these matters was always unjustified, as things were changing quickly as the virus evolved and/or vaccine efficacy devolved. Any rationale for mandating vaccines was therefore based on seriously shaky ground. And this was true even without getting into the evidence that these vaccines have a horrible safety profile (more here).
Despite all this, our government fully signaled that it would treat the science as settled on these matters, as it barreled ahead with draconian measures to coerce people into getting vaccinated. On top of that, dissenting voices were punished or censored.
Where we are today
Although some of the vaccine mandates that the Biden administration imposed were later rolled back, to this day, we still have a vaccine requirement to enter the country for non-citizens, and we still have vaccine mandates for healthcare workers and government employees, including the military.
Moreover, many universities are still mandating vaccines, and some even require boosters (examples here, here, here, here, and here), despite the fact that the young are very unlikely to have bad outcomes from COVID-19, and have the most to lose from adverse effects from the vaccines.
I hope this era of lunacy gets reflected accurately in the history books. Hopefully this timeline makes it easier for that to happen.
“Ct” stands for “cycle threshold.” During PCR, you are taking a small amount of nucleic acid (like RNA or DNA) and amplifying that small amount of starting material. You do that by running multiple “cycles” where with each cycle you have amplified it more. Ct value is the number of cycles required for the signal to cross a certain threshold. It’s inversely proportional to the amount of starting material in the sample. So a lower Ct value means that there was more nucleic acid present.
The symptoms did differ between the vaccinated and unvaccinated however:
Specifically, rhinorrhea and nasal congestion were significantly more frequent in vaccinated HCWs, while cough and fever were more common albeit not significantly in non-vaccinated subjects. Of note, when the three partially vaccinated cases were excluded from the analysis, no significant difference in these results occurred, with the exception of cough, which was less frequent in the vaccinated HCWs than in the non-vaccinated ones, in a statistically significant way.
A potential confounder here was that the median age of the vaccinated (56) was higher than in the unvaccinated (39.5). However, it’s unclear whether age affects viral load (see here).
I’ve heard people make the argument that vaccine efficacy against severe disease still led to a public benefit because it would reduce overcrowding in hospitals. I could maybe understand this more at the beginning of the pandemic but by this time there was plenty of time to ramp up hospital capacity.
Regarding the steelmanning of mandates, the goalpost shifted to include "reducing severe disease = freeing up overburdened hospital resources". Tenuous at best and a major slippery slope, but many mandate supporters did not hesitate to go here once the transmission case became weak.
Big time kudos and thanks.. timelines are so helpful & this such a beautifully referenced resource!