The way we determine SARS-CoV-2 "infectiousness" from PCR positive samples is sloppy and misleading
Vero Vero on the wall, who's the best cell line of all

PCR tests are supposed to be the “gold standard” for determining whether someone is infected with SARS-CoV-2. However, all they can do is tell you whether certain RNA sequences are present in a sample. They can’t tell you whether that RNA came from infectious “viable” virus, or non-infectious “dead” virus. In fact, the RNA might not have come from virus at all; it might have come from fragments of RNA, or defective virus-like particles that harbor incomplete viral genomes.
What we really care about when it comes to testing people, is whether and how much virus is around that’s capable of making other people sick.
There are methods that try to determine that. This article will discuss the most commonly used method, and how it can grossly mislead.
How do we commonly determine how much infectious virus is present in a sample?
The most common method for determining whether and how much infectious SARS-CoV-2 is in a sample, is to see how well the viruses in the sample can kill and grow in Vero cells, which are African green monkey kidney cells. In particular, a subline of Vero cells called “Vero E6” is most commonly used.1
Why Vero cells?
Well, they’re easy to get high amounts of virus from. This is partially because they have a genetic defect in the production of type I interferons (more here and here), which are signaling molecules that help fight viral infection.2
There are other options available for culturing SARS-CoV-2 virus, including human airway epithelial cells, which are lung cells that serve as the first barrier of defense against respiratory viruses:

Those are some of the very cells that get infected when someone catches a respiratory infection, so arguably they’d be better models for infectivity in people.
But when researchers take PCR positive samples from people and want to determine how infectious they are, they usually use Vero cells (examples here, here, here, here, here, here, here, here, here, here, and here).
How do Vero cells compare to lung cells?
How do Vero E6 cells compare with human lung cells, when it comes to susceptibility to SARS-CoV-2?
Let’s look at this study: Estimating clinical SARS-CoV-2 infectiousness in Vero E6 and primary airway epithelial cells
They found that out of 39 people who tested positive within 5 days of symptom onset, virus isolation was successful for 27 (69%) samples in Vero E6 cells, but only 12 (31%) samples in airway epithelial cells.

The human airway epithelial (HAE) cells also yielded much less virus:
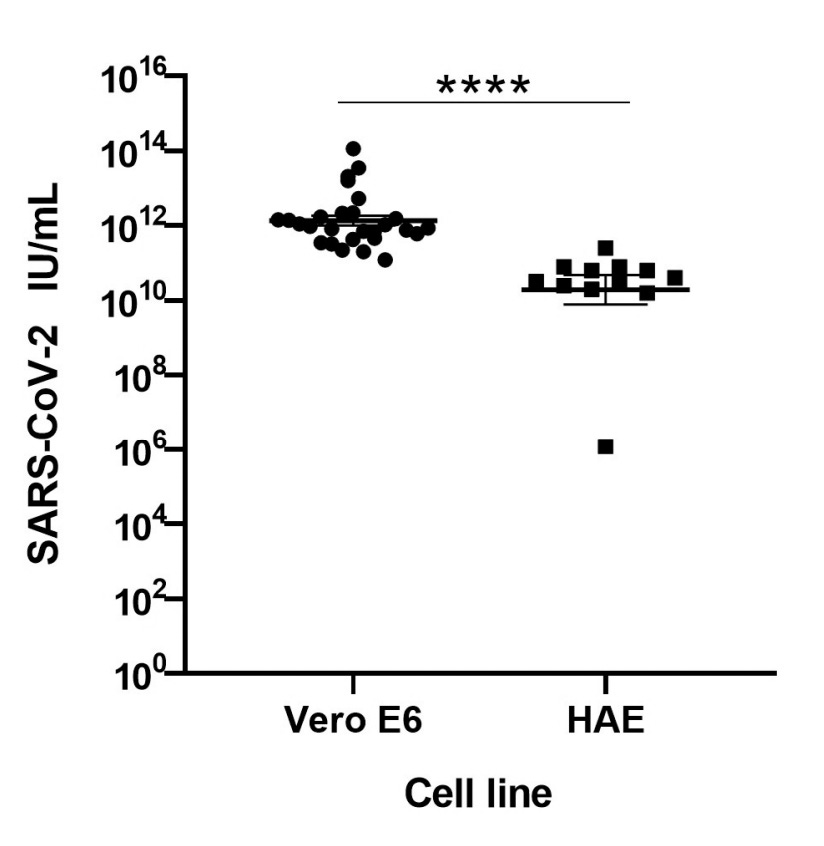
Note the scale in the graph. It’s at least an order of magnitude difference.
Now, the rationale for using Vero E6 cells, is understandable for certain use cases. For example, if one wants to produce lots of virus for some downstream application, like studying the virus itself, it makes sense.
It’s also understandable for getting a sense of how much virus is not completely “dead.” In that case, it makes sense to use a cell that is highly susceptible to the virus; that way any virus that’s still “alive” or viable can have the maximum chance of infecting a cell.
But for getting a sense of how infectious someone is to other people in real life, which is what matters for public health, it’s hard to argue that Vero E6 cells are the best cells to use. They probably overestimate what percentage of PCR positive samples contains virus that’s infectious to humans, as well as how infectious a given sample is.
All models are faulty but some are worse than others
That’s not to say that using cell cultures of human lung cells would be perfect. Any cultures, or cells grown in petri dishes or flasks, will be different from how they’d be under physiological conditions. Cell cultures wouldn’t include many things present in healthy lungs, like immune cells, antiviral proteins, and mucus, which traps and creates a hostile environment for viruses.
Other options that try to mimic the human airway or lung include organoid models, which are composed of multiple cell types, and animal models, like mice or monkeys. None of these options are perfect, but my guess is that at least some of them are better than Vero cells, at least if you’re trying to determine infectiousness to people.
What percentage of PCR positive “cases” have culturable virus?
Even with the fact that Vero cells are quite susceptible to SARS-CoV-2, often PCR positive samples don’t yield culturable virus, and the results we get are all over the place. Here’s a random sampling of studies that cultured virus from PCR positive samples:
This study found that 23 out of 129 (17.8%) patients who had both tested positive via PCR and were hospitalized with COVID-19, had culturable virus. They took 690 samples from the 129 patients, and of those, 62 (9%) had culturable virus.
This study found that 7 of 39 (18%) asymptomatic people who had tested positive had culturable virus. They took 166 samples from the 39 people, and of those, 9 (5.4%) had culturable virus.
This study found that 56 of 234 (24%) samples collected from 195 people had virus that could be isolated. The highest PCR cycle threshold (Ct) value in any sample where virus was successfully cultured was 32. Remember, higher Ct values are inversely related to the amount of starting RNA; a higher Ct value means there was lower starting amount of RNA.3
This study found that 4 out of 14 (28.6%) PCR positive patients had culturable virus.
This study found that 26 out of 90 (28.9%) PCR positive samples had culturable virus. The probability of seeing culturable virus peaked at around the third day after symptom onset, and quickly decreased after that. There was no culturable virus when the Ct value was greater than 24.
This study found that 46% (11/24) of samples at day 5 since symptom onset and 20% (6/30) of samples at day 7 since symptom onset, had culturable virus (Omicron). All the samples in this case came from vaccinated healthcare workers.
This study found that 12 of 23 (52%) PCR positive samples had culturable virus.
This study found that 6 out of 11 (54.54%) PCR positive patients had culturable virus. They also took multiple samples from the same people and they found that 15 out of a total of 63 PCR (23.80%) positive samples had culturable virus.
This study found that 29.2% of Alpha variant samples and 74.2% of Delta variant samples had culturable virus.
What should we make of these varying results?
Why the large range in results? Well, not all the protocols for sampling or culturing were the same. The types of patients sampled were not the same. The PCR tests were not all the same. The Ct values they used as cutoff points to determine whether a sample was PCR positive, were not the same. Virus variants were not the same either.
But even if we take the study reporting the highest percentage of PCR positive samples having culturable virus, which reported 74.2% of those with Delta variant having culturable virus, it’s not confidence inspiring. If we take these results at face value, it means a quarter of PCR positive patients don’t yield culturable virus.
By the way, we’ve mainly focused on methodological flaws that could lead to overestimating the infectiousness of a PCR positive sample, but there are errors that could go the other way. For example, viable virus could get stuck to the equipment used to transfer virus samples, like pipette tips,4 or samples could be stored for too long or improperly, which could lead to virus degradation and underestimating of sample infectiousness.
Do these errors balance out the bias associated with the fact that Vero cells are probably more susceptible to SARS-CoV-2 than your average healthy human? Who knows.
The main point is this: if someone says we should use a certain Ct value as a cut off point for infectiousness to humans, you should be aware that (1) they’re probably basing this on Vero cell results, and (2) the Vero cell results are all over the place.
It gets worse: co-infections are a thing
This is not the only problem. When researchers take PCR positive samples from people and culture SARS-CoV-2 from them, they’re not doing anything to try to filter out other viruses.
What they usually do is add the swab sample into a tube with enough liquid medium to spin it in a centrifuge, which separates heavier things, like cells, from lighter things, like viruses. The lighter stuff, or “supernatant” will end up on top, and this is the stuff that gets applied to Vero cells to try to kill them.
Sometimes there’s an additional filtration step, but just like with centrifugation, this just separates things by size, so there will still be other viruses present in the sample so long as they’re smaller than the filter size.
This could be a problem because Vero cells are susceptible to a whole bunch of respiratory viruses, including influenza viruses, RSV, enteroviruses, and coronaviruses. Here’s just a sampling of studies where other viruses were cultured in Vero cells:
Morphogenesis of Respiratory Syncytial Virus in a Green Monkey Kidney Cell Line (Vero)
Non-rhinovirus enteroviruses associated with respiratory infections in Peru
A previously undescribed coronavirus associated with respiratory disease in humans
Can SARS-CoV-2 PCR positive samples also contain other viruses? This gives us a clue: Rates of Co-infection Between SARS-CoV-2 and Other Respiratory Pathogens
Of the 116 specimens positive for SARS-CoV-2, 24 (20.7%) were positive for 1 or more additional pathogens, compared with 294 of the 1101 specimens (26.7%) negative for SARS-CoV-2.
Of the samples that tested positive, around 20.7% tested positive for 1 or more additional pathogens. That’s not negligible. Now, these were all in symptomatic patients (eg, cough, fever, dyspnea). Maybe the incidence is lower in asymptomatic people? But even if the incidence is half that in asymptomatic people, that’s still not a negligible number.
[UPDATE 12/15/2022: This paper reviewed multiple studies that looked at co-infections with SARS-CoV-2 and found that the pooled rate of co-infection was ~19%. The lowest reported rate of co-infections was ~3% as reported by this paper (h/t Kevin McKernan). Rates may vary for all sorts of reasons, including how researchers looked for co-infections and who they were sampling from.]
The most common co-infections were with rhinovirus/enterovirus (6.9%), RSV (5.2%), and non–SARS-CoV-2 Coronaviridae (4.3%). But it’s not like they tested for every possible virus that could be encountered in the real world; they only looked for about a dozen or so known viruses. So there could have been other viruses that weren’t checked for.
So in a nutshell, here’s what often gets done: we take swab samples from people, which may contain a multitude of viruses, and apply it to Vero cells.
In some cases, a “focus forming assay” is used to determine how much successful infection there was; this uses an antibody that’s supposed to be specific to SARS-CoV-2 to try to see how many “foci,” or clusters of infected cells are present. The benefit of this method is that so long as the antibody is truly specific to SARS-CoV-2, any foci you count should have been due to infection from SARS-CoV-2.5
However, many studies just see if applying the swab sample to Vero cells causes signs of “cytopathic effect” (CPE) or death in the cells.

After Vero cells die, some studies just attribute any cell death to SARS-CoV-2 despite the fact that other Vero-killing viruses might be present (examples here and here). This can obviously overestimate the “infectiousness” attributed to SARS-CoV-2 in the sample.
There are some studies that take further measures to at least confirm that SARS-CoV-2 is growing in the cultures, by looking for increasing levels of SARS-CoV-2 RNA (using PCR) in the cultures, for example. However, the presence of other viruses growing at the same time is not usually checked for.6 That still means that they can overestimate the "infectiousness" attributed to SARS-CoV-2 from the sample.
We should be more careful with language
There’s a sleight of hand that often happens in conversations or articles that talk about how PCR positivity translates to infectiousness. This happens because our language surrounding this topic is sloppy.7
It’s useful to make some distinctions:
We should distinguish between virus that’s “infectious to Vero cells” vs “infectious to human lung cells” vs “infectious to lung organoid models” vs “infectious to mice” vs “infectious to monkeys” vs “infectious to humans.”
“Infectious to humans” can be subcategorized further; we can differentiate between “healthy human” vs “average human” vs “the majority of humans” vs “immunocompromised human.” We should decide, from a public policy standpoint, what we care the most about, whether it’s virus that’s infectious to the “average human” or “majority of humans,” etc.
We should distinguish between virus that can kill a particular kind of cell, vs virus that can infect and replicate in that cell. That’s because it’s possible for a virus to kill a cell, or for the cell to kill itself, before the virus has a chance to replicate. In those cases, we could call the virus “cytopathic” to that cell, but perhaps we should not say it's “infectious” to that cell, if the virus isn't replicating in the cell.8
Also “infectious” does not mean the same as “transmissible,” which could further be differentiated from “transmissible in most social settings.”
For example, a virus might be able to infect a healthy person so long as you stick a bunch of the virus directly into their nose or sneeze directly into their face. You could call that virus “transmissible,” but that doesn’t mean that it has the ability to survive being in the air long enough to realistically transmit to people in most social situations, like sitting at the same table for a meal, for example.
By the way, transmissibility doesn’t just depend on properties of the virus. It will be influenced by environmental factors like temperature, presence of UV light, air flow, etc.
Key points
The way we most commonly determine whether and how much “infectious” virus is in a sample, is to culture them in Vero cells.
Vero cells have a genetic defect in the production of type I interferons which makes them particularly susceptible to viruses.
Vero cells are more susceptible to SARS-CoV-2 than human airway epithelial cells.
Use of any cell culture may overestimate infectiousness in humans because cell cultures lack many things present in healthy lungs.
Vero cells probably overestimate infectiousness more than other cell lines.
Errors that underestimate infectiousness can also occur, but we have no idea whether they balance out errors or biases that overestimate infectiousness.
Estimates of how infectious PCR positive samples are, vary a lot.
Vero cells can also host other respiratory viruses.
Co-infections with other respiratory viruses may occur at a non-negligible rate.
When we prep swab samples for culturing we don’t filter out other viruses, which means some of the cell death in cultures may be due to viruses besides SARS-CoV-2. Some methods for detecting infectiousness will over overestimate how much of the death was caused by SAR-CoV-2.
“Cytopathic” is not the same as “infectious in Vero cell” or “infectious in human lung cell” or “infectious in human lung organoid” or “infectious in a monkey” or “infectious in a healthy human” or “transmissible” or “transmissible in most social settings.”
Be wary of any stats about “infectious” virus from PCR samples
For any given PCR test, we don’t actually know what percentage of PCR positive people are also people that can make other people sick. This isn’t the same as the percentage of people that have “virus that’s culturable in Vero cells.”
Again, it’s not that we shouldn’t ever use Vero cells. For determining whether there’s any viable virus in a sample, they make sense. But we have no way of knowing whether the results we get from Vero cells come close to modeling infectiousness to humans in real life. There’s no ground truth to compare it to.
Sure, PCR can give you a sense of how much viral RNA is present, and more viral RNA may correlate with more virus that’s potentially infectious to humans.9 But if someone says things like “x amount of RNA means there is y amount of infectious virus” or “a PCR positive result with a Ct value below x means that person is likely infectious,” you should be skeptical.
You now know that they don’t really have a good way of knowing this.
P.S. This is definitely not the only problem with how we’ve been using or interpreting PCR test results; more on this will likely come in future posts.
Some studies use an engineered version of Vero E6 called “VeroE6-TMPRSS2” which is even more susceptible to SARS-CoV-2 (see here).
Interferons do this by inducing cells to do things to help limit the spread of virus, and activate immune cells, among other things (more here).
For some reason Fauci cited a Ct value of 35 as a cutoff point though. Not sure where he got that number from.
At least in part. It doesn’t mean individual cells couldn’t have been host to multiple other viruses though.
The closest thing that came to checking for this was this study which sequenced the RNA from their culture supernatants. It’s possible that other viruses were sequenced from the supernatant but the researchers didn’t try to map anything that wasn’t SARS-CoV-2, possibly because they didn’t think it was relevant to look for other viruses.
So studies that just measure whether a virus kills a particular cell culture without checking to see whether the virus is also growing in that culture, have only confirmed that the virus is cytopathic to that cell, not necessarily “infectious” to that cell.
At least early on during the course of an infection. The correlation seems to break down later during the course of an infection.
It's unfortunate that researchers and public health policy-makers sometimes fail to understand or describe transparently the limitations in the usability of analytical data for specific decision-making. This can be exacerbated by "anchoring bias" where once a test has been approved it is assumed to be the Standard and can be difficult to acknowledge its limitations or prevent its use beyond its initial intent. Your discussion highlights significant limitations in the applicability of PCR to conclude that a person IS infectious or to draw more general conclusions regarding a population. I hope in a future article you discuss examples of some limited circumstances where a significantly "biased" test may be a valuable tool. For example: you are contacted by the head of a senior care facility; a staff person has tested positive by PCR. She asks you: "should I let this staff person be around elderly persons with multiple comorbidities, or shall I assign them to other duties for a few weeks until their PCR is negative?" Let's assume the PCR has a high false positive rate (perhaps as high as 80%) but a low false negative rate (e.g., <5%), then it would be very poor at supporting a statement, "I'm confident this person is infectious." But, it might be valuable for supporting or refuting a statement, "I'm confident enough that this person is NOT infectious that I will have them work with people who are likely to die if exposed."
Joomi for President!