

Can the COVID vaccines affect athletic performance?
It doesn't look good

An interesting study that hasn’t gotten much attention
A study came out recently that should have gotten more attention. It looked at how athletes responded to getting “boosted” with the Pfizer vaccine: Effect of BNT162b2 mRNA booster vaccination on VO2max in recreational athletes: A prospective cohort study
What’s nice about this study is that they measured various markers of health before and after booster injection, in the same individuals. A total of 42 athletes were included in the study.
They found a decrease in VO₂ max post booster dose
One of the things they measured was VO₂ max both before and after booster dosing. VO₂ max is a measure of aerobic capacity; it’s the maximum rate at which the body can take up oxygen and utilize it during intense exercise. It’s an indicator of overall cardiorespiratory fitness; having a higher VO₂ max generally means you’re more fit.

Here’s what they found:
In our study, we found a statistically significant decrease in VO2max 1 week after booster vaccination with BNT162b2 mRNA. A clinically relevant decrease was found in 19% of subjects. We did not observe any major side effects from this vaccination.
More specifically they found a 2.7% decrease in VO₂ max after vaccination. In 8 (19%) of the athletes, they found a “clinically relevant” decrease of 8.6% or more.

How did 8.6% come to define “clinically relevant”? They chose that number because that’s roughly the decline in VO₂ max you’d see in men with each decade of aging. Hence, if an individual who got vaccinated went down 10 years in exercise capacity, that was considered a “clinically relevant” change.
It’s remarkable that they said “no major adverse events were observed” when they saw signs of decreased exercise capacity equivalent to ten years of aging in 19% of their participants.
Now, this decrease was seen one week after vaccination. They didn’t follow up with the athletes beyond that, so we can’t say that the booster led to any kind of long term or permanent effect on VO₂ max. However, to see a decrease like this from a shot, even if temporary, is concerning.
There were some other “side effects”
There were some other concerning things. Here’s a table which shows how many athletes had side effects:
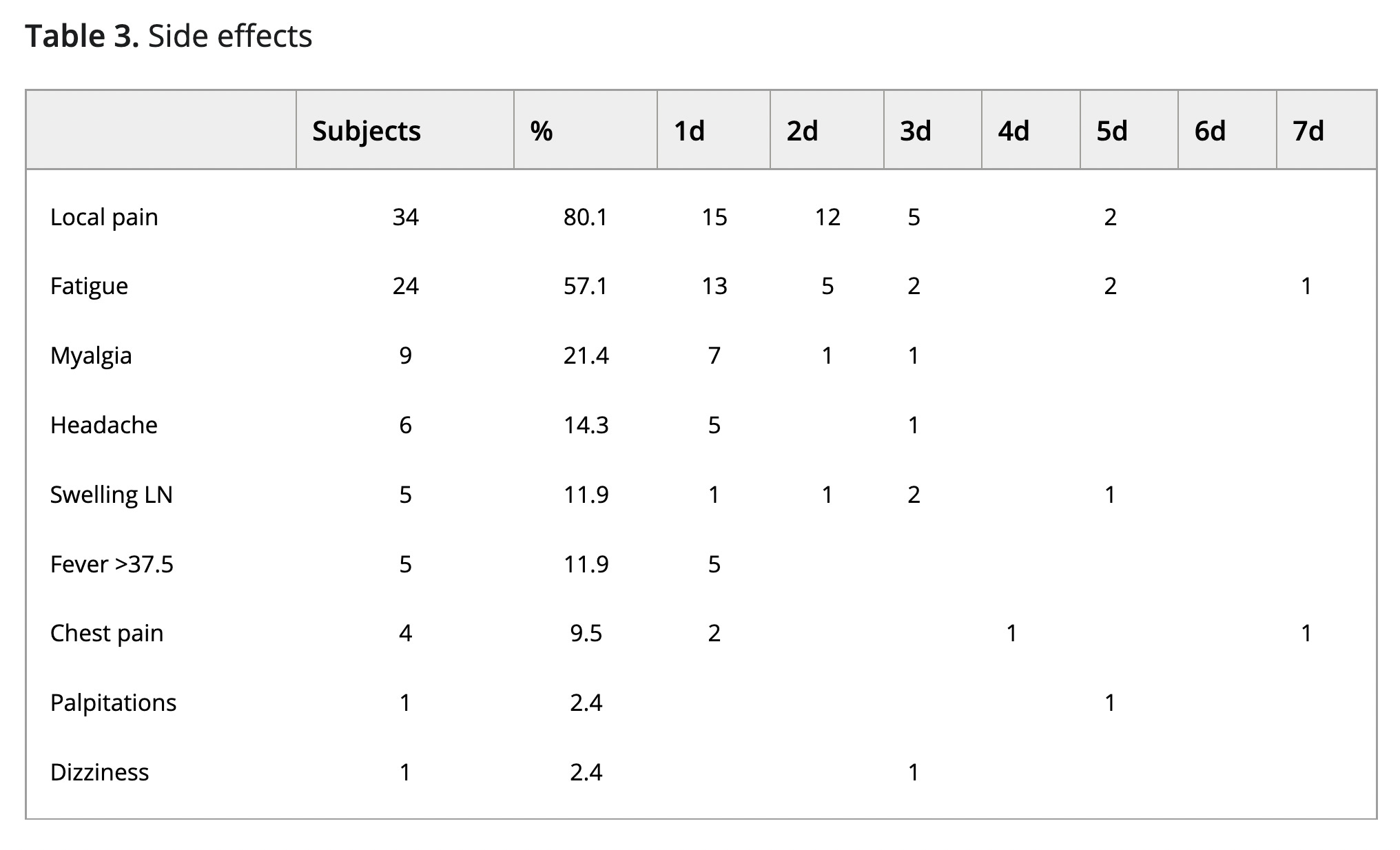
1 out of 42 had heart palpitations. 4 out of 42 had chest pain; that’s close to 10% of the participants.
What are some causes of chest pain? Well, there are various heart-related conditions like heart attack, angina, myocarditis, and pericarditis. Clots in the lungs can also cause chest pain; the FDA recently acknowledged that clots may be linked to the Pfizer shots.
But maybe some of the athletes just happened to get some muscle strains in the chest during that time. Maybe some of them just worked out a little too much. Maybe some just had acid reflux, which I hear can sometimes lead to chest pain. Or maybe some got reactivation of shingles.
Anyway, heart palpitations and chest pain should not be considered minor “side effects” from a vaccine. And yet the paper said, in its conclusion, that “No major adverse events were observed.”
At least the researchers didn’t find any obvious signs of cardiac damage, though their methods couldn’t rule out subclinical damage to the heart:
Importantly, in our small cohort of athletes, we did not see any biochemical or echocardiographic sign of (sub)clinical (peri)myocarditis after booster vaccination with the BNT162b2 mRNA vaccine. This does not fully exclude subclinical myocarditis in the absence of cardiac magnetic resonance imaging (MRI) data.
Why didn’t they do any MRIs?
As the prevalence of (peri)myocarditis postvaccination is low, we chose to not include this condition as a primary endpoint of the current study, including not performing a cardiac MRI. This results in the study being underpowered to draw firm conclusions as to the occurrence of this condition.
It’s remarkable that they said the “prevalence of (peri)myocarditis postvaccination is low.” They must be basing that on what we think we know about the prevalence in the general population, because to my knowledge no one has specifically looked at the prevalence in this demographic; adult athletes aged 18 and over. What we do know is that according to this study from Thailand, around 3.5% of boys aged 13-18 had overt or subclinical myocarditis following the Pfizer vaccine.1
The researchers did measure levels of hsTnI (high-sensitivity troponin I), which is a marker for myocardial injury. Unfortunately, they didn’t report the levels detected, or even average percentage change, though they did state that “no value over 25ng/ml” was found.
[UPDATE 12/26/2022: Correction- they did report that for hsTnI “median [IQR] pre = post 4.0 [4.0] ng/ml; p = 0.82” It would have been nice to have more granular info though.]
Something they did find was elevated hsCRP,2 which is a marker for inflammation. They found a “slight but significant increase in hsCRP” 1 week after vaccination. This isn’t that surprising because these vaccines are highly inflammatory; the lipid nanoparticles used to encase the mRNA, by themselves, are highly inflammatory.
By the way, they mentioned that one athlete “did not train at all during the week after vaccination for reasons related to the vaccination.” I hope that athlete is ok now.
Oh, and one male athlete who was originally recruited got COVID-19 immediately after his vaccination. He was not included in the results.
Did VO₂ max decrease because the athletes exercised less after vaccination?
I know what some people are thinking: is it possible that some of the athletes worked out less in the week following vaccination, and that’s what caused the decrease in VO₂ max?
In the Materials and Methods section of the paper, they mention that “Athletes were advised not to perform any intensive exercise during the first 3 days after vaccination.”
But later on, the paper states that “Most participants reported no change in their training volume or intensity in the week after their vaccination.”
Anyway, even when they only analyzed athletes who didn’t change their exercise regimen, they still saw a decrease in VO₂ max:
When only athletes who did not report a decrease in training volume and intensity (i.e., a score ≥4 for both intensity and volume [n = 22]) were analyzed, the decrease in VO2max was confirmed (from 46.1 [1.8] to 44.7 [1.8] ml/kg/min [p = 0.04]).
Besides, a decrease in training for a week or less shouldn’t be enough to see a decline in VO₂ max:
However, whereas a period of 2–4 weeks of detraining can result in a decline of VO2max, short periods of relative rest have not been shown to impact exercise capacity in well-trained athletes.
In fact, some studies suggest that modest reduction (“tapering”) of exercise shortly before an athletic competition leads to better performance.3
So my guess is that the decrease in VO₂ max wasn’t the result of some “detraining” effect.
What might be causing a decrease in VO₂ max?
VO₂ max is an important indicator of health, but it’s a very blunt tool.
It incorporates many things into one signal; like how quickly someone can take oxygen from the air into their lungs, get it into their blood, pump it into their muscles, and have the muscles use it. A decrease in VO₂ max, therefore, can be due to many different things.4
We don’t know why the Pfizer vax affected VO₂ max, but let’s briefly review some information that may be relevant to this.
Heart
We know that the LNPs, which encase the mRNA of the vaccine, don’t stay at the injection site (more here). They can end up in heart tissue and cause heart issues like (peri)myocarditis (more here, here, and here). As the authors of the study said, we can’t rule out subclinical damage to the heart.
Lungs
According to these documents that Pfizer submitted to the Japanese health authorities, the LNPs can also end up in the lungs (page 6).
Endothelial cells
The LNPs might also get taken up by endothelial cells, or the cells that line the insides of blood vessels. This could lead to inflammation and damage to the vessels, which could lead to their narrowing, which would lead to reduced blood (and oxygen) flow. There’s also evidence spike protein can cause damage to endothelial cells (see here and here).
Clots
As mentioned earlier, even the FDA has linked these shots to clots (see here and here). Clots can block small blood vessels and thereby inhibit oxygen exchange.
What’s causing the clots? Well there’s evidence that spike protein can lead to anomalous clotting in the blood. For example, this study showed that spike could lead to blood hypercoagulation (clotting), as well as changes to various proteins in the blood, like fibrinogen, a protein involved in blood clotting. These effects could interfere with blood flow, or perhaps lead to an increase in blood viscosity, or the thickness of the blood, which is inversely correlated with VO₂ max.
Red blood cells
In this video, pathologist Ryan Cole shows that applying the vaccines directly to blood causes clumping or destruction of red blood cells.5 Anomalies with red blood cells could lower VO₂ max since red blood cells are responsible for carrying oxygen throughout the body.
A big caveat: in this demonstration, Ryan Cole added about a drop of vaccine to a drop of blood. That’s a lot of vaccine to add to a small amount of blood. This is very different from what happens when someone is injected with one of these vaccines. My guess is that in people getting injected, this is probably just happening near the injection site. But I thought it was relevant to include as something to keep in mind.
Mitochondria
There’s evidence that spike protein can cause damage to mitochondria (see here or here). Mitochondria, which are frequently called the "powerhouses of the cell," are what actually consume the oxygen in our cells during the process of converting food to usable energy.
But really, we don’t know
But the damage to cells doesn’t necessarily have to be related directly to mitochondria. There are all sorts of ways that cells that have taken up vaccine could end up damaged or dead, whether they’re in the heart or lung or muscles.
All we have are guesses at this point.
As the authors of the study said:
The underlying mechanisms and clinical consequences of this finding remain unclear.
This is an understated way of saying that we have little idea of what’s going on, or what these findings mean for the long term.
If the rate of overt or subclinical myocarditis is similar in adult athletes we’d expect to see about 1.45 people in this study to have exhibited heart symptoms out of the 42 total (1.45/42 = .035). We may have seen that in this study (or more) since 1 person had heart palpitations and 4 had chest pain.
High-sensitivity C-reactive protein
Like decreased lung capacity, cardiac output, blood flow, oxygen carrying capacity of the blood, muscle metabolism, mitochondrial health, etc.
By the way, because these effects were immediate, it doesn’t seem like we can attribute them to spike protein; the cells would not have had enough time to make spike.
I wrote the corresponding author to ask whether they’d done any subset analysis of the most strongly affected cases, and whether the individual who’d had a 20% reduction in VO2Max had medical follow up. My interest was in whether there might be a gender difference in delta vo2max. The person with 20% drop got an echocardiogram which was normal. They did not do subset analysis according to the corresponding author. If you have any questions for them, I’d be happy to forward them on - I.e. more details on the participant with 20% drop
Competitive sports isn’t the place to examine this, because players on both sides have mostly been vaccinated. Track and field events have objectively stats that can be measured. Are marathon runners posting poorer times? Are long jumpers landing closer? Etc.